FDA approved for patients 2 years and older with obesity due to BBS
Help switch on the POWER of the PATHWAY™
Actor portrayals

IMCIVREE is the first and only treatment that targets impairment of the hypothalamic MC4R pathway, a root cause of hyperphagia and obesity due to Bardet-Biedl syndrome (BBS).1-3

Actor portrayals
Target a root cause of hyperphagia and obesity in BBS
Impaired MC4R pathway function2,4,5
Unlike general obesity, a root cause of obesity due to BBS is impairment of the MC4R pathway, which can occur due to ciliary dysfunction.
In people with BBS, a variant in one or more BBS genes can disrupt the BBSome.* This causes ciliary dysfunction and disruption of LEPR signaling.
Alpha-melanocyte stimulating hormone (α-MSH) production is impaired or deficient, preventing activation of the MC4 receptor.
Impairment of the MC4R pathway leads to decreased satiety signaling, hyperphagia, and reduced energy expenditure. This often leads to early-onset obesity.
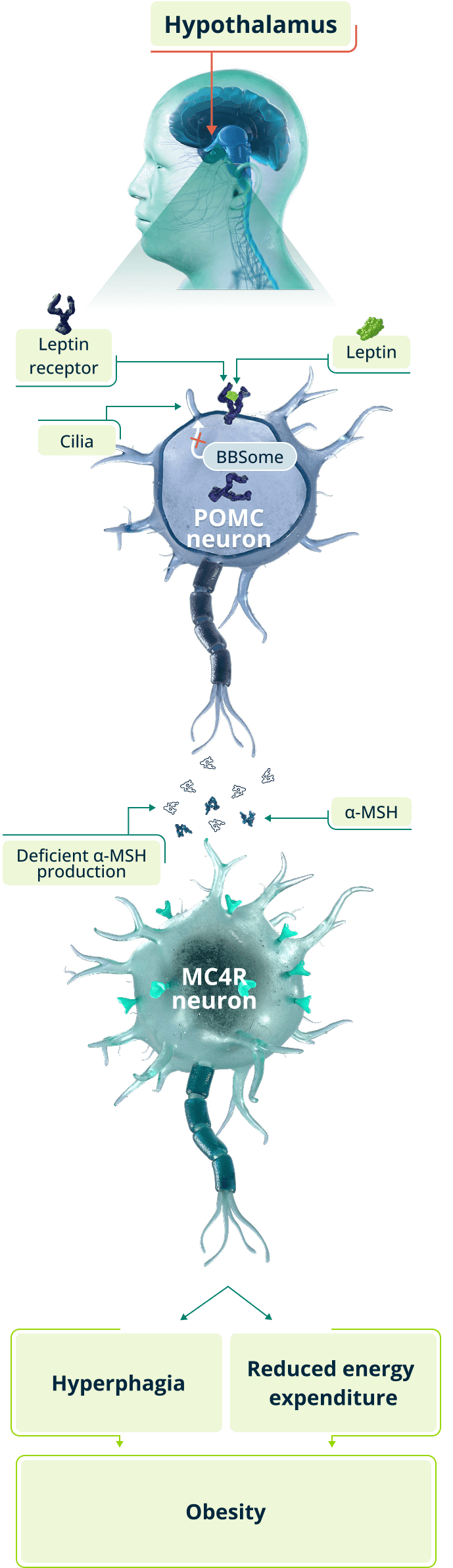
*BBSome: A complex of proteins formed by a host of BBS genes.
Reestablished MC4R pathway function1,6,7
IMCIVREE, an MC4R agonist, targets a root cause of obesity due to BBS.
IMCIVREE acts in place of α-MSH to activate the MC4 receptor and help restore MC4R pathway function.
Reestablished pathway function helps to bring hunger and satiety signals, and energy expenditure, into balance. This can lead to reduced weight.
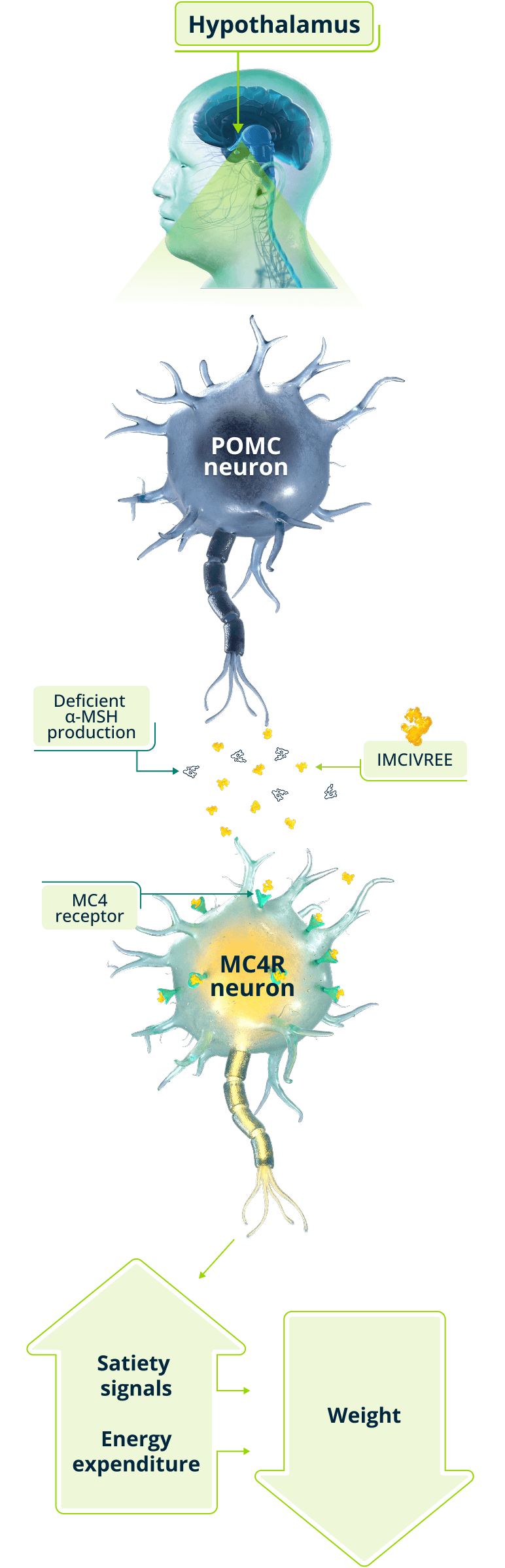
IMCIVREE helps reestablish and maintain MC4R pathway function, providing the foundation for effective long-term treatment of obesity due to BBS.1,8
About BBS2,9-12
Bardet-Biedl syndrome (BBS) is a rare autosomal recessive ciliopathy that is clinically and genetically diverse.
Along with other signs and symptoms, BBS is associated with impairment of the hypothalamic MC4R pathway. This impairment is present at birth and can lead to:
Early-onset obesity
Hyperphagia
Knowing a root cause of your patient’s hyperphagia and early-onset obesity can be an important first step in making an accurate diagnosis, which can lead to optimal management of their disease.
Explore resources for more information on diagnosing BBS in your patients.
Learn more about IMCIVREE for your patients with obesity due to BBS.
See efficacy data for IMCIVREE across age groups.
α-MSH=alpha-melanocyte-stimulating hormone, LEPR=leptin receptor, MC4R=melanocortin-4 receptor, POMC= proopiomelanocortin