Meaningful weight reduction in children

In patients 6 to <18 years old with obesity due to BBS
IMCIVREE delivered early, significant, and sustained weight reduction1,2
~8% mean BMI reduction after 1 year in children and adults 6 years and older3
The efficacy and safety of IMCIVREE for the reduction of weight and hunger in patients 6 years and older with obesity due to BBS were studied in a Phase 3 trial with a randomized, double-blind, placebo-controlled period.
BMI Z-score* Reduction in Patients 6 to <18 Years Old1,2,4†
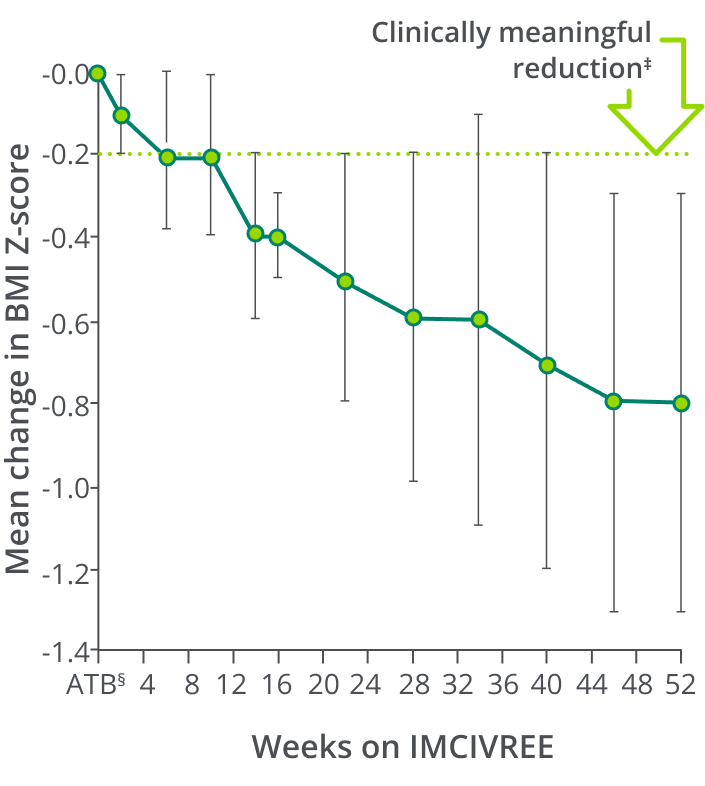
Clinically meaningful
-0.8 mean change in BMI Z-score at Week 521,2
At 24 months, patients in a long-term extension study experienced sustained mean reductions in BMI Z-score5
*BMI Z-score was an exploratory endpoint used to measure the reduction in BMI in children. A BMI Z-score is a reliable measure of weight in children who are still growing because it accounts for height, age, and gender.1,6
†Data shown include only patients who received 52 weeks of IMCIVREE at the time of the analysis. Population sizes ranged from 8 to 16, with n=14 at 52 weeks on active treatment. Error bars are the standard deviation.1
‡A clinically meaningful reduction is generally considered a ≥0.2 reduction in BMI Z-score. A 0.2 reduction is comparable to weight loss of approximately 5%.2
§ATB=active treatment baseline, defined as the last measurement before the first dose of IMCIVREE, ie, Week 0 for the IMCIVREE group and Week 14 for the placebo group.1
Individual Results in Patients 6 to <18 Years Old
Change in BMI Z-score From Baseline After 52 Weeks (n=14)4

86% of patients
achieved a clinically meaningful ≥0.2 mean reduction¶ in BMI Z-score1
100% of patients 6 to <12 years of age achieved a clinically meaningful ≥0.2 reduction in BMI Z-score (n=3).4
Patients were not required to change their diet or exercise routine.1
¶BMI Z-score was an exploratory endpoint used to measure the reduction in BMI in children. A clinically meaningful reduction is generally considered a ≥0.2 reduction in BMI Z-score. A 0.2 reduction is comparable to weight loss of approximately 5%.1,2
Change in BMI Percentile in Patients 6 to <18 Years Old1,2,7
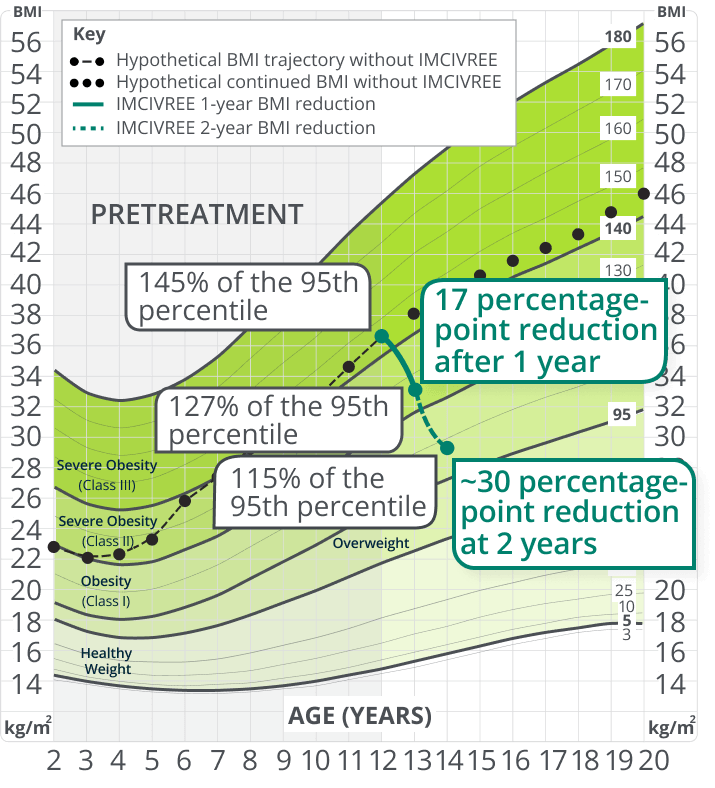
IMCIVREE significantly reduced the severity
of obesity due to BBS
This chart is a visual representation of what a hypothetical child with BBS who started IMCIVREE at age 12# may experience in BMI reduction after 1 year and 2 years, based on data from the Phase 3 trial and a separate long-term extension trial.
#Growth chart is based on females 2 to 20 years of age and is for illustrative purposes only.7
In Patients 6 to <18 Years Old
Weight Changes During the 14-week, Double‑blind, Placebo-controlled Period8
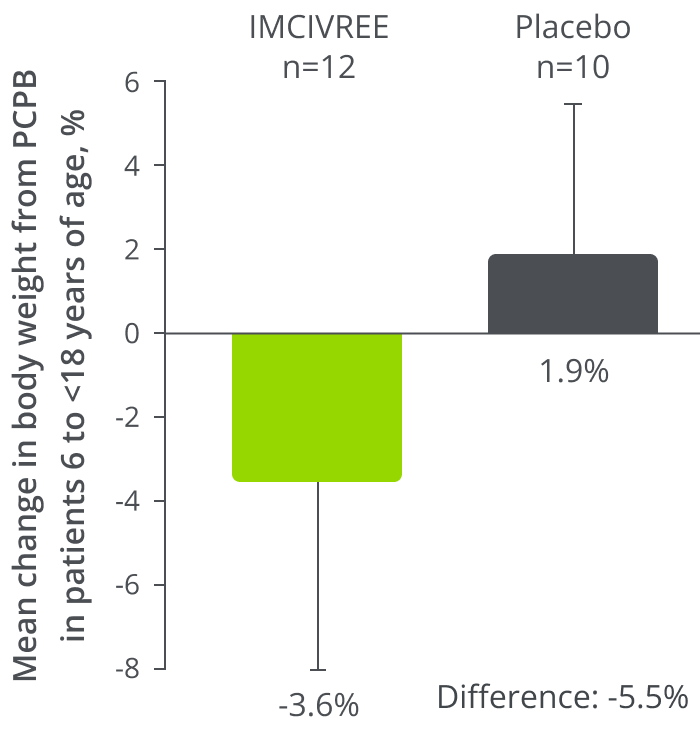
IMCIVREE reduced weight
in patients 6 to <18 years old with BBS8
Results from a combination of pivotal and supplemental patient subpopulations were based on post hoc analysis. Supplemental patients were enrolled after the pivotal cohort had begun treatment. None of the supplemental patients had completed 52 weeks of IMCIVREE treatment at the time of data analysis.1
IMCIVREE delivered sustained weight reduction at 24 months5a
0.72 average BMI Z-score reduction
after 24 months
Results from a long-term extension study in patients 6 to <18 years of age with BBS (n=12):
- At completion of an index trial, 19 patients who enrolled in a separate open-label, long-term extension study had received at least 24 months of IMCIVREE
- Patients to be assessed every 3 months until the end of the study (up to 5 years or patient withdrawal)
One patient discontinued due to an AE unrelated to IMCIVREE.
aCompared with measures at index trial baseline.
Hunger reduction in patients 12 years and older with obesity due to BBS1
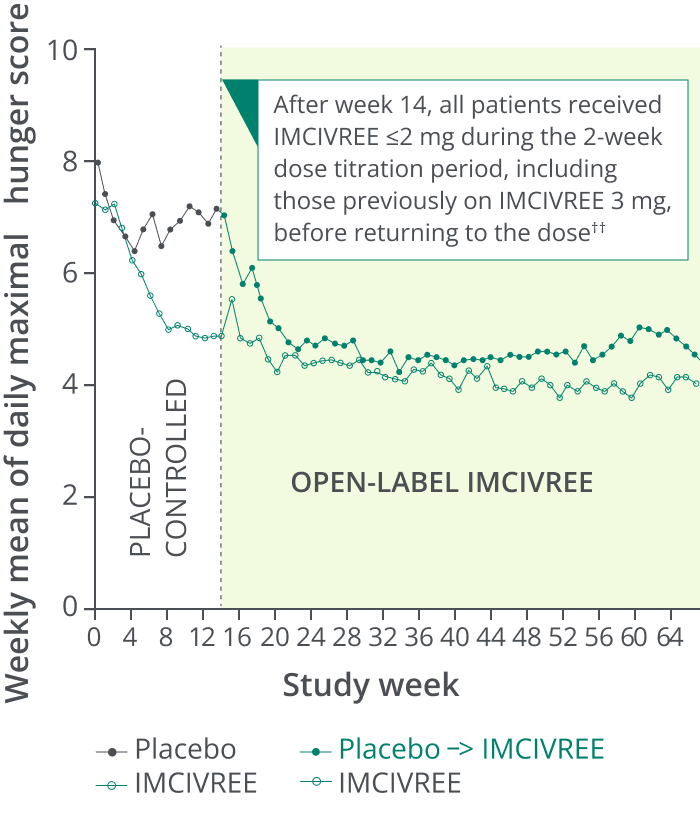
Hunger Scores in the 14-week, Placebo-controlled, and 52-week Open-label Periods8**
Clinically meaningful
2.1-point reduction
in mean hunger score
at Week 52 in patients 12 and older3‡‡
Patients who switched from placebo to IMCIVREE experienced a rapid reduction in hunger, matching that of patients initially assigned to IMCIVREE.1
Caregiver assessments were also collected for children <12 with obesity due to BBS.§§
**Patients ≥12 years of age who were able to self-report their hunger (n=14) recorded their daily maximal hunger in a diary, which was then assessed by the Daily Hunger Questionnaire Item 2. Hunger was scored on an 11-point scale from 0 (“not hungry at all”) to 10 (“hungriest possible”).3
††During the placebo-controlled period, dose titration to a fixed dose of IMCIVREE 3 mg given subcutaneously once daily was performed during the first 2 weeks of both the placebo-controlled and open-label periods to maintain blinding.3
‡‡1- to 2-point reduction is considered clinically meaningful.9
§§Data not shown.
The change in his hunger has cascaded into many positive life changes for all of us. There’s less agitation and anxiety over hunger or family meals. This is simple normalcy for many families, but for us, they’re moments I’ll never take for granted.
— Kat, caregiver of a child living with BBS
Patients and families living with BBS often express such gratitude and relief when started on IMCIVREE and see the weight trajectories and hyperphagia start to improve. To have a medication that can support correcting the biology that is dysregulated and to see positive outcomes provides hope.
– Alaina Vidmar, Pediatric Endocrinologist
Individual results may vary.
Patient-Reported Health-Related Quality of Life
In the Phase 3 trial in patients 6 years and older with BBS, PedsQL and IWQOL-Lite were assessed as exploratory endpoints and were not powered for formal statistical testing or significance. Change from baseline after approximately 52 weeks of treatment was measured by the age-specific PedsQL or IWQOL-Lite assessments.10
The PedsQL is a 23-item, self-reported, age-dependent assessment of health-related quality of life (HRQOL) in children and adolescents with or without acute or chronic health conditions encompassing 4 domain scores: physical, emotional, social, and school functioning. The total score is the mean score of the transformed items across the 4 domains. The PedsQL was administered to children 6 to <18 years of age.10,11
| PedsQL Total Scores in Patients With BBS 6 to <18 Years Old With Baseline and Week 52 Data10¶¶ | ||
|---|---|---|
| Baseline | Endpoint: Change From Baseline at Week 52 | |
| All patients (n=9) | All patients (n=9) | |
| PedsQL total score, mean (SD) | 67.2 (18.9) | +11.2 (14.3) |
- Raw scores for PedsQL were transformed on a scale of 0–100, with 0 representing the worst possible HRQOL and 100 the best possible HRQOL10
- Limitations of these results include small sample sizes across assessments, which may be in part due to the rarity of the disease10
These insights highlight the need to address hyperphagia and subsequent impaired quality of life for people with BBS and their caregivers.10
¶¶Using age-specific PedsQL assessments.10
The Impact of IMCIVREE
Hear from families and clinicians
about how IMCIVREE is bringing hope to people living with obesity due to BBS.
Get your patient started with IMCIVREE.
See efficacy data for IMCIVREE in adults.
AE=adverse event, CI=confidence interval, IWQOL=Impact of Weight on Quality of Life-Lite, PCPB=placebo-controlled period baseline, PedsQL=Pediatric Quality of Life